Excerpts from The Trigger Point Therapy Workbook by Clair Davies, NCTMB
Muscles whose trigger points cause shoulder, upper arm, and upper back pain can be divided into five groups: scalenes, shoulder blade suspension muscles, rotator cuff muscles, upper arm muscles, and spinal muscles.
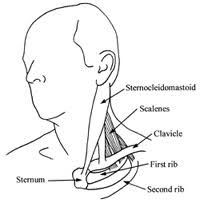
Trigger points in the scalenes cause an impressively wide distribution of pain, numbness, and other abnormal sensations in the chest, upper back, shoulder, arm, and hand. Pain is hardly ever felt in the scalenes themselves, but scalene trigger points can be the primary source of pain in their referral areas. Symptoms created by the scalenes are easily misdiagnosed. Pain sent to the shoulder by the scalenes is almost universally mislabeled bursitis or tendinitis. [There are many other symptoms and misdiagnoses listed, but I am only highlighting two, the second being carpel tunnel syndrome below.]
When trigger points shorten the scalene muscles, they tend to keep the first rib pulled up against the collarbone, squeezing the blood vessels and nerves that pass through the area on their way to the arm. The collection of symptoms caused by this compression of the nerves and vessels is properly termed thoracic outlet syndrome, although it is very often incorrectly diagnosed as carpal tunnel syndrome.
 For the complete break down on treating scalene trigger points definitely check out the Trigger Point Therapy Workbook. Know that in treating the scalene(s):
For the complete break down on treating scalene trigger points definitely check out the Trigger Point Therapy Workbook. Know that in treating the scalene(s):
This will not hurt unless you encounter a trigger point, in which case it will be extremely painful. Pressure on a scalene trigger point evokes a spooky kind of pain that will make you duck and cringe: it can feel like you're pressing on a nerve. At the same time, you may feel the referred pain or other symptom being reproduced or accentuated. This can be a very convincing demonstration of the reality of referred myofascial pain.
The massage stroke is executed by pressing with your fingertips as you push them [anterior scalene] across the muscle toward the side of the neck. The skin of the neck should move with the fingers. At the end of the stroke, which will be only an inch long, release the pressure, reset your fingers where you began the stroke and repeat. To massage the middle scalene, use this same stroke on the side of the neck. Six strokes on each scalene trigger point are enough for one session. To massage the posterior scalene, push your middle finger under the front edge of the trapezius muscle near where it attaches to the collarbone.
It's important to check for trigger points in your scalenes before going to the trouble of treating all these [rhomboids, middle trapezius, infraspinatus, latissimus dorsi, serratus anterior, and levator scapulae] other muscles. The scalenes are among the most common sources of pain along the inner edge of the shoulder blade. Without first taking care of the scalenes, massage applied to the rhomboids or to any of the others listed here, though it may feel good, can be a complete waste of time.

The supraspinatus trigger points [among other symptoms/issues] is also one of many sources of the pain in the outer elbow known as "tennis elbow". Trigger points in the triceps or one of the forearm muscles are the most usual cause of tennis elbow. Supraspinatus trigger points, being so far away and a less frequent cause, are generally overlooked as a source of this common pain (1999, 538-546). Repetitive strain such as working with the arms overhead for long periods of time or typing at a computer keyboard with no elbow support can also exhaust supraspinatus muscles. [as well as "extreme exertion, such as moving a large couch or carrying heavy weight like boxes or suitcases"....]
Paradoxically, though located behind the shoulder, infraspinatus trigger points are the most common source of pain in the front of the shoulder. This pain usually feels like it's deep in the joint and may travel some distance down the biceps. Extreme tenderness in the anterior deltoid and the bicipital groove in the head of the humerus can lead to an erroneous diagnosis of bicipital tendinitis. Pain can also shoot down the outer side of the shoulder. Occasionally, pain is referred to the back of the neck, the inner border of the shoulder blade, all the way down the upper arm and forearm, and into the entire thumb side of the hand. When pain is referred to the forearm, it tends to promote formation of satellite trigger points in the hand and finger extensors, compounding pain and other symptoms in the hand. Other symptoms of infraspinatus trigger points include weakness and stiffness in the shoulder and arm, which can cause your shoulder and arm to tire easily. Both inward and outward rotation of the arm is restricted, making it difficult to move the arm in any direction. Since arm rotation is necessary for reaching behind you, it becomes impossible to reach up behind your back. Lying on the opposite side is painful as well, because the weight of the afflicted arm pulls on the infraspinatus (1999, 556; Sola and Williams 1956, 91-95). Dysfunction of the infraspinatus typically causes the other rotators to tighten up in an effort to compensate, which tends to overload them too. All four rotators end up with trigger points and soon you're unable to move the arm at all. Nevertheless, this condition, commonly called a "frozen shoulder", can often be treated very successfully with trigger point massage of the rotator cuff muscles (1999, 552-558). [among some of the causes: keeping hands overhead for long periods of time (whether during sleep or at work), working at a computer without elbow support, keeping your hand on a computer mouse out to one side for long periods, etc.]
The infraspinatus, being on the outside of the shoulder blade, is an easy muscle to treat with self-applied massage. Confirm its location by feeling it contract and bulge as you put the arm into outward rotation. When you exert pressure on infraspinatus trigger points, the pain reaction takes awhile to wake up, so don't conclude too quickly that you have no problem there. It may take several seconds of deep massage before you feel the characteristic exquisite tenderness.
Teres minor trigger points can also be the cause of a worrisome numbness or tingling in the fourth and fifth fingers, which occurs nearly as often as the pain at the back of the shoulder. Note that a comparable pattern of finger numbness can also come from trigger points in the pectoralis minor. Pain instead of numbness in these two fingers suggests latissimus dorsi trigger points (1999, 564, 572). Teres minor trigger points are only an inch or so away from those in the infraspinatus and can be massaged at the same time with the same techniques. A tennis ball against the wall is the perfect tool: roll it slowly back and forth across the teres minor against the wall.
The subscapularis is an exceptionally powerful muscle lining the underside of the shoulder blade. Visualize it sandwiched between the shoulder blade and the ribs. You'd think that the subscapularis muscle would be unreachable and untreatable, buried as it is on the underside of the shoulder blade. Actually, it's surprisingly accessible if you go about it in the right way. This is good news, because the subscapularis is often at the very heart of the problem with shoulder pain. With a frozen shoulder in particular, knowing how to treat subscapularis trigger points can be the key to recovery; without this knowledge, recovery can be a very long time in coming (1999, 599, 603-607; Cantu and Grodin 1992, 154-155; Voss, Ionta, and Myers 1985).
The main symptom of subscapularis trigger points is severe pain deep in the back of the shoulder. An ache in the back of the wrist is almost always present and should be seen as a virtual signature of subscapularis trigger points. Sometimes the shoulder pain extends down the back of the upper arm. You may also have an extremely tender spot on the front of your shoulder where the troubled subscapularis has been continuously pulling and jerking on its attachment to the humerus (1999, 556, 600).
The pull of the four rotators must be in balance in order for the shoulder joint to operate smoothly and freely. A subscapularis muscle weakened by trigger points allows the supraspinatus to pull up on the head of the humerus unopposed, jamming it against the acromion. A clicking or popping noise when you move your shoulder indicates probable trigger points in the subscapularis or the supraspinatus, or both (1999, 545-546; Lippitt and Matsen 1998, 20-28).
Subscapularis trigger points also keep the muscle from lengthening, reducing the shoulder's range of motion and restricting rotation of the arm in either direction. This makes it difficult to reach above your head, across your body, or up behind your back. The disabling pain and stiffness caused by subscapularis trigger points are commonly mistaken for bursitis, arthritis, bicipital tendinitis, rotator cuff injury, and adhesive capsulitis (1999, 596-607).
Luckily, the most troublesome subscapularis trigger points occur near its accessible outer edge. They can be easily reached for massage if you position your arm in a way that will move the shoulder blade forward and around the side of the body. Put your hand on your opposite shoulder if possible. This pulls the shoulder blade around the side of the body and exposes a good bit of its underside. With the arm across the body, you can massage the subscapularis muscle while sitting, standing, or lying down. With the flats of your fingers firmly against your ribs, push deep into the slot between the ribs, and the roll of muscle that defines the back of the armpit. If your hand and fingers are tight against your ribs, the blunt ends of the fingers will bump right into the subscapularis. Try your thumb for this technique; you may like it better. Search for the exquisitely tender spots all along the outer edge of the shoulder blade.
The key to treating the trigger points of the shoulder/rotator cuff muscles, is to get familiar with where these muscles are, feeling around to find the trigger points, and using either thumb, fingers (with short fingernails), tennis ball, small rubber ball, or Thera Cane. Only some of the treatment suggestions are detailed in this e-mail, for a complete list/description be sure to check out the Trigger Point Therapy Workbook.
Even though I am posting excerpts from Mr. Davies' book The Trigger Point Therapy Workbook, I am by no means able to post every important facet on this subject and highly recommend you purchasing this book for your own reference...it is that good! Clair Davies' story is amazing as is his entire book. I am very grateful to his dedication and revelation of this subject matter!!!
Muscles whose trigger points cause shoulder, upper arm, and upper back pain can be divided into five groups: scalenes, shoulder blade suspension muscles, rotator cuff muscles, upper arm muscles, and spinal muscles.
Trigger points in the scalenes cause an impressively wide distribution of pain, numbness, and other abnormal sensations in the chest, upper back, shoulder, arm, and hand. Pain is hardly ever felt in the scalenes themselves, but scalene trigger points can be the primary source of pain in their referral areas. Symptoms created by the scalenes are easily misdiagnosed. Pain sent to the shoulder by the scalenes is almost universally mislabeled bursitis or tendinitis. [There are many other symptoms and misdiagnoses listed, but I am only highlighting two, the second being carpel tunnel syndrome below.]
When trigger points shorten the scalene muscles, they tend to keep the first rib pulled up against the collarbone, squeezing the blood vessels and nerves that pass through the area on their way to the arm. The collection of symptoms caused by this compression of the nerves and vessels is properly termed thoracic outlet syndrome, although it is very often incorrectly diagnosed as carpal tunnel syndrome.
This will not hurt unless you encounter a trigger point, in which case it will be extremely painful. Pressure on a scalene trigger point evokes a spooky kind of pain that will make you duck and cringe: it can feel like you're pressing on a nerve. At the same time, you may feel the referred pain or other symptom being reproduced or accentuated. This can be a very convincing demonstration of the reality of referred myofascial pain.
The massage stroke is executed by pressing with your fingertips as you push them [anterior scalene] across the muscle toward the side of the neck. The skin of the neck should move with the fingers. At the end of the stroke, which will be only an inch long, release the pressure, reset your fingers where you began the stroke and repeat. To massage the middle scalene, use this same stroke on the side of the neck. Six strokes on each scalene trigger point are enough for one session. To massage the posterior scalene, push your middle finger under the front edge of the trapezius muscle near where it attaches to the collarbone.
It's important to check for trigger points in your scalenes before going to the trouble of treating all these [rhomboids, middle trapezius, infraspinatus, latissimus dorsi, serratus anterior, and levator scapulae] other muscles. The scalenes are among the most common sources of pain along the inner edge of the shoulder blade. Without first taking care of the scalenes, massage applied to the rhomboids or to any of the others listed here, though it may feel good, can be a complete waste of time.
The supraspinatus trigger points [among other symptoms/issues] is also one of many sources of the pain in the outer elbow known as "tennis elbow". Trigger points in the triceps or one of the forearm muscles are the most usual cause of tennis elbow. Supraspinatus trigger points, being so far away and a less frequent cause, are generally overlooked as a source of this common pain (1999, 538-546). Repetitive strain such as working with the arms overhead for long periods of time or typing at a computer keyboard with no elbow support can also exhaust supraspinatus muscles. [as well as "extreme exertion, such as moving a large couch or carrying heavy weight like boxes or suitcases"....]
Paradoxically, though located behind the shoulder, infraspinatus trigger points are the most common source of pain in the front of the shoulder. This pain usually feels like it's deep in the joint and may travel some distance down the biceps. Extreme tenderness in the anterior deltoid and the bicipital groove in the head of the humerus can lead to an erroneous diagnosis of bicipital tendinitis. Pain can also shoot down the outer side of the shoulder. Occasionally, pain is referred to the back of the neck, the inner border of the shoulder blade, all the way down the upper arm and forearm, and into the entire thumb side of the hand. When pain is referred to the forearm, it tends to promote formation of satellite trigger points in the hand and finger extensors, compounding pain and other symptoms in the hand. Other symptoms of infraspinatus trigger points include weakness and stiffness in the shoulder and arm, which can cause your shoulder and arm to tire easily. Both inward and outward rotation of the arm is restricted, making it difficult to move the arm in any direction. Since arm rotation is necessary for reaching behind you, it becomes impossible to reach up behind your back. Lying on the opposite side is painful as well, because the weight of the afflicted arm pulls on the infraspinatus (1999, 556; Sola and Williams 1956, 91-95). Dysfunction of the infraspinatus typically causes the other rotators to tighten up in an effort to compensate, which tends to overload them too. All four rotators end up with trigger points and soon you're unable to move the arm at all. Nevertheless, this condition, commonly called a "frozen shoulder", can often be treated very successfully with trigger point massage of the rotator cuff muscles (1999, 552-558). [among some of the causes: keeping hands overhead for long periods of time (whether during sleep or at work), working at a computer without elbow support, keeping your hand on a computer mouse out to one side for long periods, etc.]
The infraspinatus, being on the outside of the shoulder blade, is an easy muscle to treat with self-applied massage. Confirm its location by feeling it contract and bulge as you put the arm into outward rotation. When you exert pressure on infraspinatus trigger points, the pain reaction takes awhile to wake up, so don't conclude too quickly that you have no problem there. It may take several seconds of deep massage before you feel the characteristic exquisite tenderness.
Teres minor trigger points can also be the cause of a worrisome numbness or tingling in the fourth and fifth fingers, which occurs nearly as often as the pain at the back of the shoulder. Note that a comparable pattern of finger numbness can also come from trigger points in the pectoralis minor. Pain instead of numbness in these two fingers suggests latissimus dorsi trigger points (1999, 564, 572). Teres minor trigger points are only an inch or so away from those in the infraspinatus and can be massaged at the same time with the same techniques. A tennis ball against the wall is the perfect tool: roll it slowly back and forth across the teres minor against the wall.
The subscapularis is an exceptionally powerful muscle lining the underside of the shoulder blade. Visualize it sandwiched between the shoulder blade and the ribs. You'd think that the subscapularis muscle would be unreachable and untreatable, buried as it is on the underside of the shoulder blade. Actually, it's surprisingly accessible if you go about it in the right way. This is good news, because the subscapularis is often at the very heart of the problem with shoulder pain. With a frozen shoulder in particular, knowing how to treat subscapularis trigger points can be the key to recovery; without this knowledge, recovery can be a very long time in coming (1999, 599, 603-607; Cantu and Grodin 1992, 154-155; Voss, Ionta, and Myers 1985).
The main symptom of subscapularis trigger points is severe pain deep in the back of the shoulder. An ache in the back of the wrist is almost always present and should be seen as a virtual signature of subscapularis trigger points. Sometimes the shoulder pain extends down the back of the upper arm. You may also have an extremely tender spot on the front of your shoulder where the troubled subscapularis has been continuously pulling and jerking on its attachment to the humerus (1999, 556, 600).
The pull of the four rotators must be in balance in order for the shoulder joint to operate smoothly and freely. A subscapularis muscle weakened by trigger points allows the supraspinatus to pull up on the head of the humerus unopposed, jamming it against the acromion. A clicking or popping noise when you move your shoulder indicates probable trigger points in the subscapularis or the supraspinatus, or both (1999, 545-546; Lippitt and Matsen 1998, 20-28).
Subscapularis trigger points also keep the muscle from lengthening, reducing the shoulder's range of motion and restricting rotation of the arm in either direction. This makes it difficult to reach above your head, across your body, or up behind your back. The disabling pain and stiffness caused by subscapularis trigger points are commonly mistaken for bursitis, arthritis, bicipital tendinitis, rotator cuff injury, and adhesive capsulitis (1999, 596-607).
Luckily, the most troublesome subscapularis trigger points occur near its accessible outer edge. They can be easily reached for massage if you position your arm in a way that will move the shoulder blade forward and around the side of the body. Put your hand on your opposite shoulder if possible. This pulls the shoulder blade around the side of the body and exposes a good bit of its underside. With the arm across the body, you can massage the subscapularis muscle while sitting, standing, or lying down. With the flats of your fingers firmly against your ribs, push deep into the slot between the ribs, and the roll of muscle that defines the back of the armpit. If your hand and fingers are tight against your ribs, the blunt ends of the fingers will bump right into the subscapularis. Try your thumb for this technique; you may like it better. Search for the exquisitely tender spots all along the outer edge of the shoulder blade.
The key to treating the trigger points of the shoulder/rotator cuff muscles, is to get familiar with where these muscles are, feeling around to find the trigger points, and using either thumb, fingers (with short fingernails), tennis ball, small rubber ball, or Thera Cane. Only some of the treatment suggestions are detailed in this e-mail, for a complete list/description be sure to check out the Trigger Point Therapy Workbook.
Even though I am posting excerpts from Mr. Davies' book The Trigger Point Therapy Workbook, I am by no means able to post every important facet on this subject and highly recommend you purchasing this book for your own reference...it is that good! Clair Davies' story is amazing as is his entire book. I am very grateful to his dedication and revelation of this subject matter!!!
No comments:
Post a Comment